Student Name
Capella University
NURS-FPX9010 Doctor of Nursing Practice 2
Professor Name
Submission Date
Project Proposal
It is essential that outpatient telepsychiatric services be an integral part of aftercare in order to provide continuity of care, optimize treatment outcomes, and reduce the risk of relapse for psychiatric patients. Many outpatient psychiatric services are also hampered by the inconsistent follow-up of patients. This problem negatively affects treatment outcomes and increases the utilization of emergency services (Hugunin et al., 2023). The independent outpatient psychiatric clinic where the project is being implemented has a 25% baseline rate of patients following up within 30 days after an appointment, which is significantly less than the national standards, which are 35.3% within 7 days and 50.7% within 30 days of an encounter (Simple Practice EHR dataset, Nov. 03, 2025, internal site; Medicaid.gov, 2026). There is an increasing level of telepsychiatry, and due to an absence of a consistent system of reminders or follow-up, patients will likely become disengaged from the clinic (Clinical Director, Nov. 3, 2025, personal communication). The project’s PIOCT is: In an outpatient telepsychiatry clinic (P), what is the impact on patient follow-up adherence rates (O) from implementing a telepsychiatry follow-up protocol with a reminder system, as recommended by the CPSTF (I), compared to current practices (C), within a period of 12 weeks (T)? This quality improvement project aims to provide the nursing staff of the telepsychiatry unit with an evidence-based telepsychiatry follow-up protocol, with reminders, and offers a goal of increasing follow-up adherence to a minimum of 20%, thereby improving continuity of care and outcomes for clients.
Practice Problem
The practice problem identified for the practicum site arose from the November 2025 electronic health record data regarding the 30-day follow-up. This data indicated a 30-day follow-up adherence rate of 25%, whereas the national average was 50.7% (Clinical Director, personal communication, November 3, 2025). Several issues related to the practicum site processes were identified, including a) the absence of a systematized reminder process, b) a predominantly manual and opportunistic follow-up process, and c) a lack of engagement with patients post-telepsychiatry session. The clinic treated 40-60 patients per week, and even though there was some use of telepsychiatric services, it still had the problem of patients dropping out of care. The clinic had around 40 to 60 patients per week, and there was some usage of telepsychiatry, but no efforts to ensure continued engagement, which led to patients being lost. The local problem echoed the general pattern of the nation, which was recorded in literature. There was still a problem with initial adherence in settings, with studies showing 59.4% of psychiatric outpatients had completed timely return visits within 30 days (Chen et al., 2022). Additionally, less than 10% of the patients of state-funded facilities received recommended follow-up within 30-days of discharge (Hermer et al., 2021). The results highlighted the importance and need for systematics in the context of patient follow-up in psychiatric care settings.
One of the most basic elements of good healthcare – all day, everywhere – is continuity of care. Since the start of the COVID-19 pandemic, mental health issues across the country have worsened, and research has proven that psychiatric complications, such as anxiety, depression, cognitive deficits, and even the development of psychiatric diseases, have been observed after COVID-19 infection (Taquet et al., 2021; Poletti et al., 2021; Taquet et al., 2022). Sadly, national-level data show troubling trends – the number of outpatient mental health visits and the number of psychotropic medications used by adolescents and young adults have almost doubled from 2006 to 2019, reflecting growing mental health needs and the growing demand for psychiatric services (Horst & Bourgeois, 2024). Mental health service use was markedly impacted by the pandemic: providers reported major changes in the number of contacts with patients, and a rise in the number of consultations regarding post-COVID syndromes (Czeisler et al., 2021; Fehr et al., 2024). Access to early outpatient follow-up (OPT) post psychiatric discharge was shown to have a significant effect in reducing suicide risk, especially by patients with substance use disorder, schizophrenia, bipolar disorder, and depression (Ee et al., 2023). Treatment engagement was improved with effective care management programs, but barriers such as transportation issues, financial instability, and lack of availability of mental health professionals remained in all settings.
Project Site
The project site is a privately owned outpatient psychiatric clinic located in an urban environment. As an ambulatory organization, its primary focus is on the provision of assessment, psychotherapy, use of psychiatric medications, and follow-up services to adult patients with mental illness whose primary symptoms include depression, anxiety, and bipolar disorder. (Clinical Director, personal communication, November 3, 2025). The outpatient mental health clinic has 5 or fewer support staff, a psychiatric nurse, therapeutic staff, and staff who help with scheduling and billing. There are 2 psychiatric nurse specialists who assist with patient follow-up and psychiatric continuity. (Simple Practice EHR dataset, internal site, November 03, 2025). The clinic draws an attendance of 40-60 patients a week, 30 of whom receive services in the clinic, while 10 to 30 receive services through teletherapy. The clinic is located in a diverse, urban community. It is likely that outpatient mental health services are needed by a high proportion of the community’s residents. Socioeconomic and structural barriers in the community may limit levels of follow-up.
Project Fit for DNP Site
This site makes an ideal choice as part of the DNP practicum for various contextual and organizational reasons. The clinic’s increasing reliance on telepsychiatrists since the Covid-19 pandemic provides an ideal opportunity to install the practice-based, evidence-synthesized digital reminder, along with the structured follow-up procedures (Clinical Director, personal communication, November 3, 2025). The small size and integrated nature of the clinic’s staff greatly contributed to the adoption, development, and further refinement of the procedures. The clinic’s location in the inner city and its range of clientele, coupled with the persistent problems of OPPs of forgetfulness, variability, and ambivalence, suggest that reminder systems, especially those employing text messaging, would greatly improve psychiatric appointment attendance. Given that the organizational perception of the follow-up rate and absence of a structured procedure leaves significant room for improvement, the size, clientele, and practice and organizational structure suggest that this site represents an ideal opportunity for the implementation of procedures to improve outcome measures and the follow-up rate in telepsychiatry.
Current Ineffective Practice
Anxiety, depression, and bipolar disorder are examples of chronic psychiatric conditions. Barriers to regular follow-up care include staff reliance on patients to either self-initiate follow-ups or increase their follow-up frequency, or to do no more than send a ‘reminder’ message or call when the clinician is free. Current practices show a lack of standardized follow-up. About 25% of patients have an outreach response within a 30-day window (Simple Practice EHR dataset, internal site, November 03, 2025). There is insufficient proactive outreach and monitoring. This causes patients to be at risk for not being fully engaged, and increases their risk for psychiatric symptoms to worsen, and to frequently need to go to the Emergency Department (ED). This is particularly concerning with a Tele-Psychiatry model because there is an increased risk of no-shows. Inconsistency and lack of follow-up are time and cost-adversive to the clinician. They negatively impact the continuity of psychiatric care and increase the risk of patient relapse and ED utilization.
Support for Organizational Strategic Initiatives
The organization is focusing on optimizing telepsychiatry services, improving quality, and promoting patient engagement, all of which this program supports. The Clinical Director stated that the program being proposed will directly support these (3) facets by creating a telepsychiatry visit follow-up plan and establishing a visit reminder system. This will enable the clinic to provide the telepsychiatry service in an easy, timely, and high-quality manner. The program outcomes will contribute to the organization by addressing the following: reducing the no-show rate, increasing the staff’s time, energy, and skill/knowledge level, and reducing avoidable visits to the emergency department and subsequent hospital re-admissions. The program’s proposed follow-up improvement goals, driven by a 20% increase from current levels, and additional goals for follow-up improvement within 30 days (from current levels), when met, will significantly increase the clinic’s compliance with the national benchmark (50.7%) for follow-up appointment adherence within 30 days, and will demonstrate the clinic’s commitment to quality and evidence-based practices (Medicaid.gov, 2026). Finally, this program supports the clinic’s strategic initiative and goal to achieve a competitive advantage in the current marketplace by improving the clinic’s reputation for whole-person care.
Previous Projects Addressing the Problem
Prior to the DNP project, the organisation had not systematically assessed compliance or set up a reminders system that is evidence-based. Site leadership reported that there has never been a formal, structured quality improvement project that focuses specifically on follow-up adherence of patients in telepsychiatry (Clinical Director, personal communication, November 3, 2025). On a few occasions, individual staff have tried interventions with parents or carers, but it was not a consistent process, did not have an impact over time, and was not effective. There has not been a previous structured project—a challenge and opportunity, as there is no baseline intervention data available for comparison, yet there is organizational readiness and motivation for evidence-based quality improvement projects. The DNP project will serve as a basis for future performance monitoring, data-informed decision making, and an iterative quality improvement process for improving patient engagement and continuity of care in the telepsychiatry model of service.
Project Population
The design and implementation of an intervention are dependent on an understanding of the target population. Project population will comprise nursing staff working in an outpatient telepsychiatry clinic who will implement the standardized follow-up protocol and reminder system. The nursing staff will comprise two psychiatric nurse specialists who are already providing help for patients in follow-up and psychiatric continuity of care. All nurses will be engaged in similar career positions with direct care responsibilities and care coordination, making appointments and monitoring symptoms, and conversing with therapeutic language with adult patients having chronic psychiatric illnesses, such as depression, anxiety, and bipolar disorders. Studies showed that providing a clear description of the target population (who they are and what they are) creates more relevance to the intervention, and makes it more likely to succeed (Capili, 2021). The clinical experience of the nursing staff will vary, and they will be providing the majority of clinical care via telepsychiatry with some face-to-face interactions. All participating nurses will be working with adult patients (18 years old and older) who will need continuing psychiatric follow-up care within 8-10 weeks since their last encounters. The population composition will ensure the appropriate implementation of the interventions and measurement of outcomes.
Inclusion and Exclusion Criteria
Clearly-defined participant criteria facilitate creating the right sample of participants and valid outcome measurement in quality improvement initiatives. Inclusion criteria will include all nursing staff at the outpatient psychiatric clinic who work directly with the patients, are involved in their scheduling, provide follow-up communication, and are involved with the adult patient receiving telepsychiatry services for a chronic psychiatric condition. Staff members involved will gain access to the EHR system, attend staff training on the standardized follow-up protocol, and will have a regular clinical schedule during the 12-week implementation. Including and excluding can improve a QIP’s internal validity by reducing selection bias and creating uniform participants (Jensen et al, 2025). Exclusions will apply to staff who hold only administrative positions with no patient contact, staff on leave throughout implementation, temporary or contract staff who will not be a part of this project in its entirety, and staff who do not engage with the telepsychiatry service delivery. These considerations will improve the uniformity of the procedures and the continuous collection of data throughout the project.
Minimum Participant Requirements
Appropriate sample size (for evaluation of efficacy of intervention, generalizability of the results to similar clinical contexts). At least 2 of the nursing staff at the practicum site will need to be involved in the project and have to use a reminder system to implement the standardized telepsychiatry follow-up protocol. Currently, the outpatient psychiatric clinic has two psychiatric nurse specialists to help with follow-up and continuity of care (CPS), which equals the minimum number of participants required to implement the project. Each nurse will be able to attend to around 40-60 patients/wk, which will allow for adequate patient encounters for follow-up adherence measurements and assessment of the effectiveness of the intervention during the 12-week implementation. In small clinical settings, quality improvement projects can be effective with a sample size that matches the nature of the quality improvement and the metrics measured (Wittich et al., 2024). Data collection will take place in formative intervals via the Simple Practice EHR system over the 12-week implementation period, to capture follow-up adherence rates, no-show percentages, and documentation completion rates in Weeks 4, 8, and 12. The nursing staff will keep a formal record on a template basis of reminder outreach attempts and systematically track outcomes of attempts to contact patients. The learner will be completing the Weekly EHR audit to make sure all data is complete and accurate, and the implementation logs will document contextual factors and barriers to adherence outcomes during the intervention period. The practice site, therefore, will have the necessary staffing and census to support the implementation of the project and assessment of outcomes.
Evidence-Based Interventions
Solid evidence base that shows clinical usefulness and practicality in a variety of settings is necessary for effective implementation of healthcare interventions. Both the asynchronous and synchronous modalities were found to yield similar clinical results, and both led to statistically and clinically significant improvement in patients’ functioning in the primary care setting (Yellowlees et al., 2021). Likewise, when looking at PCP adherence with psychiatrist recommendations made after telepsychiatry visits, there were no significant differences between the different telepsychiatry modalities, and both were found to be feasible and acceptable for the provision of collaborative psychiatric care (Lieng et al., 2021). Use of the short message service (SMS) did not have a significant effect on stroke prevention knowledge, although there was some evidence of improved medication adherence among patients with chronic conditions (Aigbonoga et al., 2025). Based on the findings, telepsychological services resulted in a decrease in psychological distress in COVID-19 survivors, and participants reported a high satisfaction level for telepsychological services (Khademi et al., 2023). Alongside telecom strategies, an automated booking system for appointment confirmation significantly reduced the ‘no show’ phenomenon in mental health clinics (19.85% to 7.01%); therefore, employing all existing approaches for automated digital reminders was essential (Brancewicz et al., 2025). When taken together, the primary agile offerings demonstrated the usefulness of technology-based psychiatric post-treatment methodologies in a wide array of treatments.
In the remaining psychiatric groups, digital reminder systems combined with telecom-based follow-up consistently improved patient engagement and clinical outcomes. Hamlin et al. (2023) found that mobile apps enhanced adherence and engagement to treatment when users were reminded daily and when users visually tracked their progress. Similarly, text message reminders for pediatric populations saw statistically significantly higher attendance of their appointments when compared to standard of care, with the effectiveness of these text messages being highest for medical appointments as opposed to vaccines (Tan et al., 2024). However, transdiagnostic stepped-care delivered through telehealth showed feasibility in the treatment of emotional disorders in children, where collaborative decision-making procedures were used to guide decisions for treatment levels of care (Kennedy et al., 2021). Community mental health organizations that adopted and implemented tele-psychiatry services experienced benefits that were in line with the telehealth effectiveness research findings (Mahmoud et al., 2021). These organizations noted significant patient engagement, an increased patient population, greater overall efficiency in the delivery of services, less time wasted by patients in the waiting lines, and positive feedback from patients, family, and staff. In particular, the 12-month structured tele-medicine follow-up procedure significantly reduced the incidence of suicide attempts and the number of attempts significantly in the tele-medicine follow-up group, who reattempted suicide the least, and those who reattempted had the longest waiting time in comparison to the usual care control groups (Otiñano et al., 2025). Evidence-based interventions have proven successful in an even greater range of psychiatric disorders, and with varying patient populations.
There was consistent support in the literature for structured telecommunication interventions and their effectiveness in bettering psychiatric continuity of care and patient outcomes. Regarding primary care physicians’ adherence to the psychiatrist’s recommendations after the telepsychiatry consultation, no major differences were noted between the asynchronous and synchronous methods, in addition to both methods being viable and well accepted for the collaborative offering of the psychiatric services (Lieng et al., 2021). More beneficial outcomes were associated with SMS interventions, where high medication adherence in intervention groups showed a 14.7% increase compared with a 2.7% increase in the control groups, which showed no statistically significant difference between groups (Aigbonoga et al., 2025). Automated phone calls and text messaging systems used to remind individuals to fill out forms have achieved return rates of 55.41%, with individuals aged 35-44 responding the best (Brancewicz et al., 2025). Digital, automated systems that assist in follow-up care help foster improved relationships between physicians and their patients, especially when physicians engage with these systems; however, engagement may be negatively impacted by the user’s depression severity (Hamlin et al., 2023). Telecommunication-based interventions showed that structured follow-up care delivered over a 12-month period had a 54% lower risk of undelivered care compared to other support interventions (Otiñano et al., 2025). Evidence found that structured telepsychiatry follow-up systems utilizing reminder systems showed clear integration of telecommunication methods for structured engagement of telepsychiatric services within the psychiatric group.
Implementation Plan for Interventions
The goal is stepwise implementation over 12 weeks for consistency in both implementation and outcome measurements. The learner will combine educational sessions for staff scheduled for the first week, and staff scheduled for follow-up telepsychiatry. Education for staff scheduled for telepsychiatry sessions will include the reminder system and their documentation in the EHR. Competency assessments for manual reminder outreach will be performed during the 72- and 24-hour periods prior to scheduled appointments, using simulated patient scenarios. Nursing staff will be required to demonstrate competency to perform the outreach. A reminder system will be used to strengthen appointment adherence systems. There are numerous telecommunication follow-up systems that enhance patient engagement, as well as sustain and improve patient care. Staff will perform manual reminder outreach during the 72- and 24-hour periods prior to scheduled appointments. Staff will document all their outreach attempts in the EHR. The learner will be monitoring adherence and will address any implementation issues. The learner will document follow-up with the preceptor each week and with the stakeholders every two weeks. Evidence demonstrates that structured reminder systems significantly improve appointment adherence rates across psychiatric populations (Brancewicz et al., 2025). In week 12, data will be extracted, final outcome analysis will be performed, comparing pre- and post-intervention follow-up adherence rates, and stakeholder feedback will be collected to evaluate the project. The project’s primary outcome measure is the percentage of the total number of patients who attend a scheduled telepsychiatry visit within 8–10 weeks of an initial meeting. Baseline adherence of 25% will be compared to post-intervention adherence, with the goal of at least 20% adherence to the national 30-day post-intervention adherence rate of 50.7%. Secondary outcomes include no-show rates and EHR documentation completion rates for reminder outreach attempts.
Learner Role and Preceptor Partnership
The learner will be the academic leader and take charge of planning, executing, assessing, and sharing results of the 12-week intervention. Weekly meetings with the preceptor will involve discussing progress, addressing issues, planning data collection, and discussing compliance with the organization. The learner will communicate status updates via progress reports prepared every two weeks, and meetings to discuss progress with the medical director of psychiatry, nurse supervisor, and telehealth coordinator, as well as the quality improvement specialist. The learner will also engage stakeholders through email and meetings. Successful outcomes of evidence-based care management programs depend on ongoing monitoring and collaboration with other fields of healthcare, as well as at the interdisciplinary level (Connor, 2023). The learner will use detailed project implementation checklists to monitor timely adherence to the project, perform weekly electronic health record audits for timely data collection, prepare formative analyses at Weeks 4, 8, and 11 to evaluate early signs of patient follow-up rate changes, and make adjustments to project implementation strategies that arise from analysis findings and support the goal of achieving a 20% increase in patient follow-up rates.
InInternal and External Stakeholders
If different groups of stakeholders are going to be engaged and collaborate effectively throughout the implementation process, they need to be talking to one another and having a meaningful conversation around healthcare initiatives. Multiple internal and external stakeholders will be active and directly affected by the intervention in the project. Involvement will include the outpatient behavioral health clinical manager who can serve as preceptor, the medical director of psychiatry who will oversee the administration of the program, the nurse supervisor who will coordinate staff, the telehealth coordinator who will help manage the technical aspects of the program, the quality improvement specialist who will ensure the program adheres to standards, and the nursing staff who will implement the standardized follow-up protocol including reminder systems. Adult patients receiving telepsychiatry services will be external stakeholders and will benefit from enhanced communication and continuous care. Stakeholder engagement strategies directly affect the implementation success and sustainability of evidence-based interventions (Triplett et al., 2022). Collaborative care models rely on a fully active participation of the interdisciplinary team in the treatment of the patient, with each member of the team providing the care in order to reach the best outcome for the patient (Kongkar et al., 2025). The stakeholders will be involved via weekly and fortnightly meetings, giving feedback on barriers to implementation, following newly introduced reminder procedures, and participating in the outcome evaluation system to keep on improving the quality.
Interprofessional Team Members
Successful quality improvement projects are based on teamwork within inter-professional teams where all team members have complementary skills and have defined roles. The interprofessional team will be made up of various professionals with a healthcare background and specialized expertise in various fields to assist in the implementation and evaluation of the project. The psychiatric nurse practitioner will offer clinical consultation on patient assessment protocols, medication management considerations, and patient symptom monitoring procedures that will require immediate clinical escalation. This manual appointment scheduling, reminder outreach communication, and documentation of follow-up attempts will be implemented by two psychiatric nurse specialists who will be the primary intervention implementers and monitor the way patients engage throughout the 12 weeks. The telehealth coordinator will help with technical questions regarding telepsychiatry platforms, assist with troubleshooting connectivity, staff training regarding virtual visits, and stay abreast of telehealth compliance. Interdisciplinary collaboration in mental health care leads to better service quality and greater satisfaction of clients (Bendowska & Baum, 2023). Collaborative care models improve engagement with treatment as well as clinical outcomes across a variety of psychiatric populations (Reist et al., 2022). Administrative staff will assist in navigating the functions of the system for scheduling, verifying patient demographics, and correcting entries in the system, and a quality improvement specialist will assist with the implementation of process improvements within the organization.
Data Collection, Analysis, and Desirable Outcomes
Across healthcare practices, systematic data gathering and rigorous assessment ensure valid metrics and facilitate evidence-based changes in practice. The most pertinent outcome relates to the increase in the percentage of patients attending follow-up telepsychiatry appointments within the 8-10 week period. This percentage increase is anticipated to be a minimum of 20% based on data collected from the telepsychiatry clinic’s EHR system. Adherence to the 30-day follow-up (Medicaid.gov, 2026) will be compared to the current (2025) adherence rate of 25%, and will demonstrate the improvement toward the national baseline (2026) of 50.7% adherence. The application of evidence-based reminder interventions has been documented in thousands of studies of psychiatric populations and consistently produces a significant reduction in no-shows and improvement in retention of appointments. The no-show rate (percent of no-shows of total scheduled appointments) and rate of completion of documented contact (percent of scheduled contacts documented) will be regarded as secondary outcomes. Evaluation will be based on the protocol compliance of nursing staff (weekly audits will be conducted, looking at reminder outreach documentation) and the success rate of the contact with the patient, determined as the percentage of patients reached through reminder communications.
They use valid and reliable measurement tools to accurately assess outcomes and to be able to interpret the results of a quality improvement project. There will be no other measurement tools needed, as follow-up adherence will be based on scheduling and encounter data that can be directly extracted from Simple Practice’s EHR system.
A pre/post intervention comparison design will assess the intervention’s effectiveness by comparing data from November 2025 (baseline) with data collected at Weeks 4, 8, and 12. Basic descriptive statistics will include the calculation of percentages to express follow-up adherence and no-show rates, as well as adherence to documentation at baseline and post-intervention, and the calculation of percentage point differences to show the magnitude of improvement between baseline and post-intervention. Follow-up adherence and no-show rates, as well as adherence to documentation, will be expressed as percentage point differences to show the improvement between baseline and post-intervention. Structured outcome measures (OMs) capture telecommunication-based psychiatric interventions (Yellowlees et al., 2021). Many mental health initiatives incorporate sustained quality improvements and systematic data collection and analysis (Nwobodo et al., 2024). This will allow the learner to create frequency tables to summarize patient demographic data, as well as collect and present continuous data to stakeholders in a format that facilitates sustained decision-making, like a graph that displays data on the mean time between patient appointments.
Conceptual Model
Quality Improvement Frameworks are systematic methods of testing and implementing changes with evidence in healthcare settings that result in measurable improvements in outcomes. The plan-do-study-act (PDSA) model, as its name states, is an iterative framework that allows for the testing of change, learning from the results, and modifications of the process to improve and perpetuate the interventions. (Chen et al., 2021). Using the PDSA method to solve problems systematically creates an environment of designed experiments and data-based decisions that fosters continuous improvement and learning while minimizing the risks associated with process implementation. The ‘plan’ phase of the project will include setting specific project aims to increase adherence from 25% to 45% on telepsychiatry follow-up adherence; establishing a standardized telepsychiatry follow-up protocol with reminder systems; identifying who in the nursing staff will be responsible; identifying how to collect the data; and predicting outcomes based on baseline measurements of adherence at 25%. In the ‘do’ phase, the intervention protocol will be carried out during a period of 12 weeks, and nursing staff will perform manual reminder outreach and record follow-up attempts, and real-time data on adherence patterns and implementation barriers experienced during daily functioning will be collected.
PDSA Integration with Project Goals and PICOT
Quality improvement frameworks integrated with the objectives of specific projects can promote strategic project implementation and allow for the evaluation of meaningful outcomes during the various stages of the project. The ‘study’ phase will involve analysing the collected data at Weeks 4, 8, and 12 by calculating follow-up adherence percentages, comparing them with adherence percentages at baseline, identifying trends in no-show rates, checking adherence to documentation, and evaluating barriers identified by nursing staff during weekly checks with stakeholders. The ‘Act’ phase will involve making changes in reminder timing, changing the types/content of reminders based on feedback from patients, changing the way documentation is done to improve workflow, identifying challenges in implementation and taking action to resolve these challenges, in collaboration with relevant stakeholders, and deciding upon implementing either as is or adapting or discarding specific protocol elements for ongoing implementation beyond the project life span. Iterative cycles of quality improvement facilitate ongoing improvement of evidence-based interventions (Kittelman et al. 2021). The use of a framework to guide implementation improves both the effectiveness of intervention and the adoption of best practices (Eboreime et al., 2021). If there are some actions that need to be improved to make the intervention more effective at achieving the target 20% improvement in patient adherence outcomes, then multiple PDSA cycles may be performed.
Methodology, Budget, and Ethical Considerations
Assumptions shape strategy and influence expected outcomes in health service improvement efforts. This project assumes that nursing staff comply with the standardized protocol, that patients have functional phone numbers, that the electronic health record (EHR) has accurate appointment scheduling, and that leadership will continue to be supportive (Alzghaibi & Hutchings, 2024). The project will incorporate a pre/post intervention design, excluding a control group, to assess adherence to the follow-up protocol post intervention. The implementation of the follow-up protocol will be evaluated in order to assess the implementation of the follow-up protocol. There are a number of frameworks to evaluate practice change in the psychiatric setting (Connor, 2023). Rigid intervention protocols enhance the reliability of outcome measurements. This will be achieved using a non-experimental design. A primary focus of this design is the enhancement of the practice, and the intent aligns with more traditional frameworks of quality improvement, where the focus is on a receptive, transformative process within the organization, and an elevation of the organizational performance.
Project Limitations and Mitigation Strategies
Research and improvement projects have inherent limitations. This project’s limitations include a lack of control group for making causal claims, a small sample size, a short duration of the project, which may be insufficient to assess long-term sustainability, potential distorting factors in patient attendance (e.g., seasonal factors), a possible external factor in attendance, and the use of existing EHR data without established measuring tools (Alomar et al., 2024). To reduce these limitations, several iterations of the project will include a developing analysis, implementation logs documenting contextual factors and barriers to implementation, and collection of qualitative data from both nursing staff and patients regarding the acceptability and feasibility of the improvement initiative (Fontaine et al., 2024). Validating the quality of an improvement initiative requires a rigorous documentation approach. Recognizing limitations, gaps, or uncertainties will not only provide a qualitative benefit to the improvement initiative but also guide future iterations and implementations.
Project Budget
Sustainable support for evidence-informed interventions in health care organizations is facilitated by allocating resources according to meticulous budget planning. In the project budget, we will aim to minimize costs associated with the existing clinic infrastructure. This will include the existing EHR system, nursing staff with pre-scheduled shifts, and the clinic’s existing telecommunications system. Estimated costs will account for partial FTE nursing staff for training and outreach, and nursing staff for project management and data analysis (considered a donated service), time spent attending multiple meetings, and potential changes to EHR for improved reporting. Sufficient resources are critical to the success of quality improvement efforts (Tyler & Glasgow, 2021). Open and clear budgets are essential for gaining support and ensuring planning for the sustainability of the organization (Ballesteros & Bisogno, 2022). The focus of our estimated total costs will be on decreasing the organization’s costs, while ensuring the greatest possible effect of the intervention and the sustainability of future growth.
HIPAA Compliance and Data Security
Patient confidentiality and data security are integral components of healthcare quality improvement, and this is an ethical responsibility in any such quality improvement effort. The project will remain HIPAA compliant using a variety of strategies to ensure the de-identification of all patient data during analysis, including eliminating names, medical record numbers, and other identifiers from patient data. Moreover, their innovative approach includes assigning patient records with distinct numerical tracking codes, allowing only the project team members who complete HIPAA training to access the information (Subramanian et al., 2024). There will be a combination of various means of physical and cyber security, such as the use of electronic devices with passwords and automated time-out features, files backed up and stored on secure organizational servers, along with locked offices and secured laptops (Duan et al., 2025). Privacy protection measures may pose challenges, but they will ensure that the quality improvement projects will be undertaken with the utmost ethical regard. Upon the conclusion of the project, all data pertaining to the project will be deleted as stated in the organizational policy.
Project Timeline
The implementation timeline will be broken down into a detailed 12-week step-by-step account of the major activities and milestones for each project phase to ensure systematic implementation of the project outcomes. Standardized telepsychiatry program follow-up protocols will be introduced to all nursing staff participants during education sessions over Week 1. Protocols for reminder system procedures and EHR documentation will also be addressed. Weeks 2-3 will include staff competency assessments along with simulated patient training. Workflow integration strategies will also be completed to improve nursing staff readiness to deliver interventions. In Week 4, the full set of protocols will be implemented. Formative assessments of intervention delivery will be used to review adherence, and baseline data will be collected. Methods will be adjusted to address early implementation challenges. Improvement in the organization of a project is a benefit of a structured implementation. Improvement of phased project design aids the gradual incorporation and refinement of evidence-based standards. For Weeks 5-7, nursing staff will continue to deliver the support. Weekly checks will be conducted by the preceptors, and barriers will be documented. In Week 8, the second formative assessment will take place, and stakeholder feedback will be obtained. Protocols will be adjusted at this point in the implementation to address stakeholder input. Weeks 9-11 will see the continued delivery and high levels of oversight and intervention. Week 12 will be the final data collection, in-depth assessments of impact and engagement with stakeholders to discuss plans for sustained impact.
The full implementation plan for the quality improvement project is documented along with the timeline in Appendix C.
Figure 1
Gantt Chart of Project Work Plan and Timeline
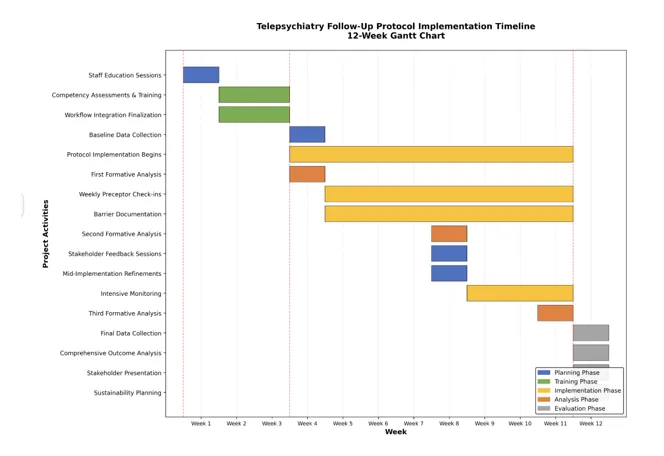
Note. It visualizes the week-by-week breakdown of tasks and activities over the 12-week implementation period.
Practicum Hours Plan of Action
DNP 1,000 Practicum Hour Plan Of Action | |||
Transfer Hours – Please indicate if they have been approved or submitted. | |||
DNP Project Hours | Approved transfer hours from core courses | 510 | |
Hours completed in NURS 9000 | 0 | ||
Projected hours from NURS 9010 | 0 | ||
Subtotal Transfer Hours | 510 | ||
Practicum Hours | Course | Activity | Planned hours |
NURS9020 | Extract baseline data on follow-up adherence, no-show behaviors, reminder documentation practices, and patient demographics from the Simple Practice EHR system for the outpatient psychiatric clinic. | 50 | |
Meet with relevant stakeholders, such as psychiatric nurse specialists, the psychiatric medical director, the nurse supervisor, the telehealth coordinator, and the quality improvement specialist, to validate the project scope and assess the feasibility of the research protocols and the integration of the workflows. | 40 | ||
Perform a comprehensive environmental scan of current practices for follow-up, workflows for scheduling telepsychiatry appointments, reminder systems, EHR documentation templates, staffing capacity, and communication resources. | 50 | ||
Develop a standardized telepsychiatry follow-up protocol, including reminder timing guidelines (72 hours and 24 hours pre-appointment), communication scripts, documentation templates, troubleshooting procedures, and patient engagement strategies. | 30 | ||
Full proper data management planning, HIPAA compliance analysis, patient privacy protection procedures, data security protocols, and ethics alignment for quality improvement project activities | 45 | ||
Start nursing staff interviews and competency assessments to identify training needs, implementation barriers, workflow challenges, and support requirements for delivering standardized telepsychiatry follow-up with reminder systems. | 40 | ||
Make staff training curriculum materials, including protocol manuals, quick-reference guides, simulation scenarios, competency checklists, and implementation logs for systematic reminder outreach procedures. | 50 | ||
Join preceptor planning meetings each week to monitor progress of implementations, review preliminary adherence data, address emerging barriers, refine intervention procedures, and adjust project timelines. | 45 | ||
Total | 350 | ||
NURS9030 | Conduct extensive employee training on the implementation of a standardized telepsychiatry follow-up protocol, manual reminder outreach techniques, telephone communication strategies, and electronic health record documentation procedures. | 50 | |
Oversee nursing staff and their use of systematic manual reminders. This includes sending reminder communications 72 and 24 hours prior to appointments, documenting attempted contacts, and tracking the patient’s response. | 50 | ||
Offer ongoing staff consultation addressing complex patient situations, with disconnected telephone numbers, patient resistance, appointment rescheduling requests, and technology troubleshooting for telepsychiatry platforms. | 50 | ||
Hold a weekly meeting with the nursing staff to assess the remaining fidelity for the implementation, identify difficulties in meeting the workflow, help with any questions about documentation, and give tailored assistance for adherence to the protocol. | 50 | ||
Execute systematic chart reviews evaluating reminder documentation completion, follow-up attempt quality, patient contact success rates, and adherence to standardized protocol procedures throughout the implementation period. | 50 | ||
Assist with bi-weekly stakeholder meetings to present initial outcome data, discuss the progress of implementation, identify organizational barriers, and receive feedback on the acceptability of the protocol and necessary modifications. | 50 | ||
Participate in interdisciplinary coordination activities, including communication with the medical director, collaboration with the telehealth coordinator, consultation with the quality improvement specialist, and engagement with administrative leadership. | 50 | ||
Total | 350 | ||
NURS9040 | Execute formative outcome evaluations at Weeks 4, 8, and 11, examining follow-up adherence percentages, no-show rate trends, documentation completion metrics, and preliminary progress toward 20% improvement goal. | 100 | |
Based on your input and staff feedback, adjust reminders, communication, documentation, staff workflows, and strategies for protocol implementation between Plan-Do-Study-Act cycles. | 50 | ||
Analyze the results thoroughly by comparing the baseline 25% adherence rate with the new rates after the implementation. Determine the percentage point improvement, assess if the target outcomes were achieved, and evaluate the secondary metrics, including no-show rates and the quality of documentation. | 50 | ||
Develop dissemination materials, including an executive summary report, a stakeholder presentation with tables and graphs, a project poster for an organizational quality improvement showcase, and a manuscript draft for professional publication. | 50 | ||
Work with leadership to integrate standard procedures for telepsychiatry follow-ups. This will involve the formal integration of actionable clinical operations, the establishment of regular review practices, and the planning and resourcing of staff training and new employee orientations. | 50 | ||
Total | 300 | ||
Total Practicum Hours | 1,000 | ||
Conclusion
The initiative aims to bridge a significant discontinuity concern in psychiatric care. This involves integrating a novel, evidence-supported, tele-psychiatry follow-up procedure in conjunction with a screening appointment reminder system, the latter of which is to be embedded within the nursing staff. This 12-week initiative aims for a minimum 20% increase in follow-up appointment attendance from a baseline value of 25%, thus coming closer to the national average of 50.7% (Goal 0). Based on the plan-do-study-act design, the project will iterate nurse reminder outreach, explaining and examining the results through formative analyses conducted during the outreach cycles. Once the reminder system is in use, it will offer ongoing, proactive tele-psychiatry appointment reminder outreach. This will increase patient involvement, reduce the patient-nurse communication gap, and accommodate optimal tele-psychiatry clinical outcomes.